The Omega-3 Index: The Blood Test That Tells You If Your Fish Oil Is Actually Working
Most people taking fish oil have no idea whether it's actually doing anything inside their body. They guess. They hope. They keep taking it because someone told them to, or because they read something a few years back. There is a simple blood test — small enough to do at home with a finger prick — that turns all of that guesswork into a single, actionable number. It's called the Omega-3 Index blood test, and it's quietly become one of the most useful biomarkers in longevity medicine.
What the Omega-3 Index Actually Measures
The Omega-3 Index measures EPA and DHA — the two main marine omega-3 fatty acids — as a percentage of the total fatty acids present in your red blood cell membranes. That's it: one number, expressed as a percentage. The reason it works so well is that red blood cells turn over every three to four months, which means the test isn't picking up what you ate yesterday or the capsule you took this morning. It's giving you a running average of how much EPA and DHA your tissues have actually been absorbing over the past several months.
Think of it as the omega-3 equivalent of HbA1c — the long-term blood sugar test used to monitor diabetes. Both are stable, both reflect real tissue status, and both ignore the noise of any single meal or day. That stability is what makes the Omega-3 Index so valuable.
This distinction matters because standard plasma omega-3 testing — the cheaper, more common option — bounces around wildly depending on whether you've recently eaten salmon or taken a capsule. A plasma result can look perfectly respectable while your tissue stores are quietly depleted. The Omega-3 Index doesn't mislead you in that way. It tells you what's actually there.
What's a Good Omega-3 Index Number?
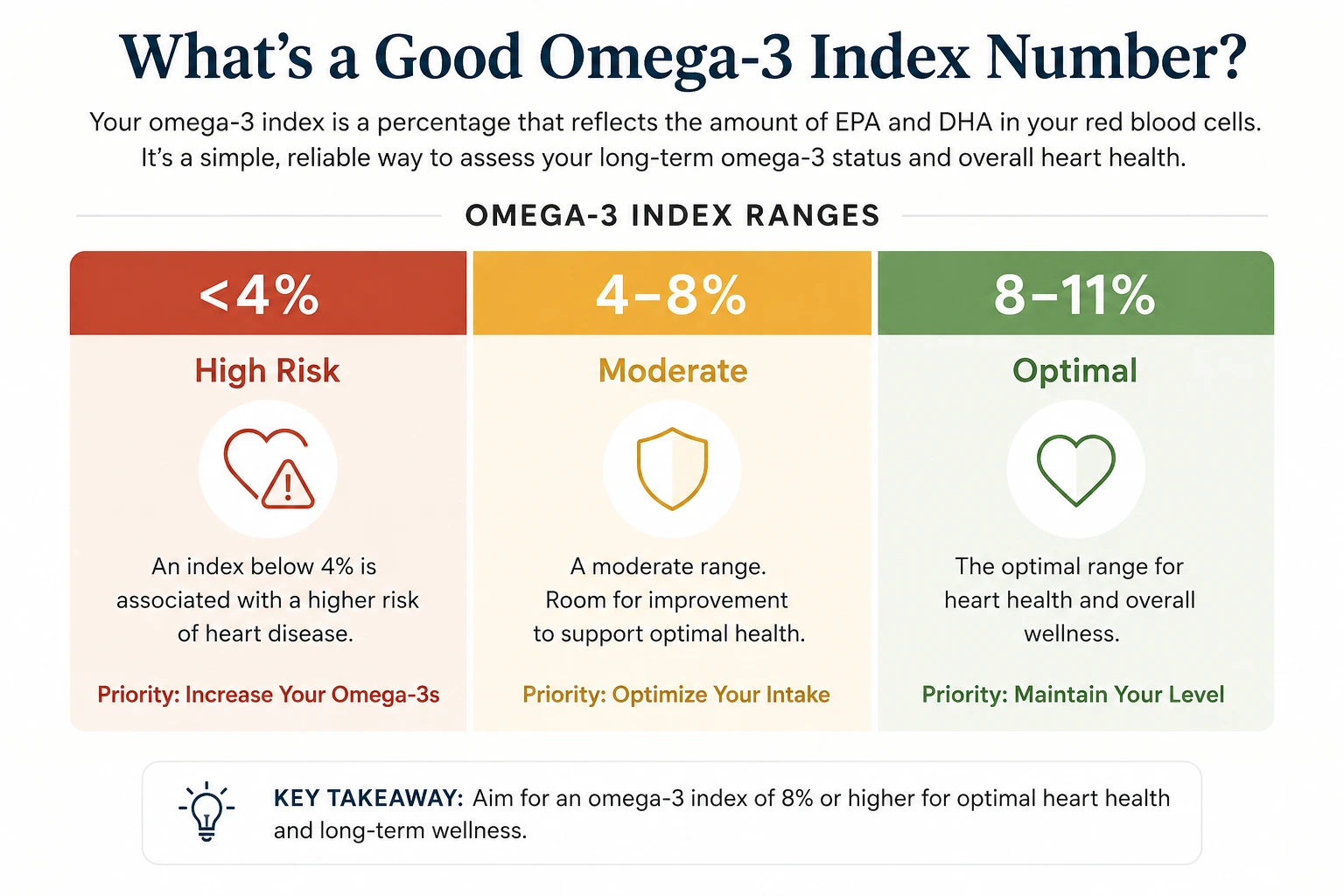
The Omega-3 Index was first proposed as a cardiovascular risk marker by researchers William Harris and Clemens von Schacky in a 2004 paper in Preventive Medicine. Their framework, built from observational data on sudden cardiac death, has held up remarkably well across two decades of follow-up research. The current consensus looks roughly like this:
Below 4% is the high-risk zone. Observational studies have consistently linked an index in this range to higher cardiovascular event rates and elevated all-cause mortality. In one analysis of 65-year-olds, an Omega-3 Index under 4% carried roughly the same 10-year mortality risk as being a current smoker.
Between 4% and 8% is the intermediate zone — common, but not where you want to stay. The majority of adults in the US and UK sit here. Average American levels hover around 4 to 5%; in the Framingham Offspring cohort, the mean was 5.6%.
Between 8% and 11% is the desirable target range. This is roughly where Japanese populations sit on average (around 8.5%), and it's associated with the lowest cardiovascular event rates in the original Harris and von Schacky framework. Most researchers cap the upper recommended target at around 11%, as benefits appear to plateau beyond that point.
It's worth noting that these cutoffs come from cardiovascular risk modelling — they're not strict diagnostic thresholds the way an HbA1c reading for diabetes is. A result of 3.8% in a healthy 30-year-old means something quite different from the same number in a 60-year-old with elevated triglycerides and a family history of heart disease. The Omega-3 Index is one piece of the picture, and an important one, but not the whole picture.
The average American has an Omega-3 Index of around 4 to 5%. The average Japanese adult sits closer to 8 to 9%. That gap maps almost too neatly onto the differences in cardiovascular disease rates between the two countries — one of the clearest illustrations of how a single dietary pattern can shift an entire population's risk profile.
Why This Test Belongs in a Longevity Routine, Not Just a Cardiology Workup
The Omega-3 Index started life as a heart marker, but the research has steadily expanded. In a recent review of more than 450 studies citing the index in their title or abstract, it had been used to investigate cognition, mood, pregnancy outcomes, exercise recovery, immune function, and brain volume in older adults. The general pattern across all of this: a higher index is associated with more favourable outcomes in most areas studied.
Two things stand out from a longevity perspective. First, EPA and DHA aren't just floating around as fuel — they're structural components of brain cells and retinal photoreceptors. Tissue levels matter for how those cells signal and function, and the Omega-3 Index is the only widely available test that reflects tissue levels rather than recent intake.
Second, the index is modifiable. Unlike age or genetics, it responds reliably to changes in diet and supplementation, typically within three to four months. That makes it one of the more satisfying biomarkers to track over time: measure, adjust, re-measure, see whether it worked. Very few longevity markers offer that kind of clean feedback loop.
How to Take the Omega-3 Index Blood Test — and Improve Your Score
Testing is straightforward. Most labs offer a finger-prick kit you can do at home — a few drops of blood onto a card, posted back, results in around two weeks. There's no fasting required, no phlebotomist needed, and the cost typically falls somewhere between £40 and £80 in the UK or $50 and $100 in the US, depending on whether you also request a full fatty acid profile or trans fat panel.
If your result comes back below 8%, the practical path forward is consistent daily EPA and DHA intake. The research-supported dose for moving the index meaningfully sits in the range of 1 to 2 grams of combined EPA and DHA daily, taken with a meal that includes some fat to support absorption. Triglyceride-form fish oils tend to absorb more efficiently than ethyl ester forms — a distinction that matters more than most of the branding on the bottle.
Re-test at three to four months. That is the minimum time needed for red blood cells to fully reflect any change you've made. Testing sooner than that gives you a moving target and, often, unnecessary frustration. The index moves slowly because it's measuring something real.
One quiet, useful insight from the research: the same supplement dose can produce very different responses in different people. Body weight, starting status, absorption efficiency, and the form of oil all play a role. This is precisely why the test exists — to replace assumption with evidence.
What's in the Supplement
- Harmover Omega-3 EPA & DHA Softgels Each softgel delivers 180 mg of EPA and 120 mg of DHA from concentrated fish oil, stabilised with vitamin E to protect against oxidation. For someone working to move their Omega-3 Index from a typical Western baseline into the desirable 8–11% range, two softgels taken twice daily with meals provides 1.2 g of combined long-chain omega-3 — a dose that sits comfortably within the range shown to shift the index meaningfully over three to four months. Manufactured in the USA.
- Eicosapentaenoic Acid (EPA) One of the two long-chain marine omega-3 fatty acids measured by the Omega-3 Index. Once incorporated into cell membranes, EPA serves as the raw material for resolvins and other pro-resolving mediators — signalling molecules that help your body resolve inflammatory processes cleanly. EPA is the omega-3 most strongly associated with the cardiovascular outcomes that motivated the original development of the index, including effects on triglycerides, blood pressure, and inflammatory markers.
- Docosahexaenoic Acid (DHA) The structural half of the equation. Your body preferentially deposits DHA into brain cell membranes and the photoreceptors of the retina, where it shapes how those cells signal and function. EFSA has approved health claims recognising that DHA contributes to normal brain function and normal vision at a daily intake of 250 mg, and that DHA combined with EPA supports normal heart function. Both fatty acids contribute to your final Omega-3 Index score.
Common Questions
What is the Omega-3 Index blood test?
The Omega-3 Index blood test measures EPA and DHA — the two key marine omega-3 fatty acids — as a percentage of the total fatty acids in your red blood cell membranes. Because red blood cells turn over every three to four months, the result reflects your actual tissue status over time, not just what you ate recently. It's a more reliable picture of your omega-3 levels than a standard plasma test.
What is a good Omega-3 Index score?
The desirable target range is 8–11%. Below 4% is considered high risk. Most adults in the US and UK sit in the 4–8% intermediate range. Japanese populations, who eat significantly more oily fish, average around 8.5% — and their cardiovascular disease rates reflect that gap.
How do I raise my Omega-3 Index?
Consistent daily intake of EPA and DHA is the most reliable way to raise your score. Research supports 1–2 grams of combined EPA and DHA per day, taken with a meal containing some fat. Triglyceride-form fish oils absorb better than ethyl ester forms. Re-test after three to four months — that's the minimum time for your red blood cells to fully reflect the change.
How often should I test my Omega-3 Index?
Test once to establish your baseline, then re-test three to four months after making a change to your diet or supplementation. Once you're in the 8–11% target range, an annual check is sufficient for most people.
If you've been taking fish oil for years and never tested, you're flying blind. That's not a criticism — almost everyone is. But of all the longevity biomarkers you could measure, the Omega-3 Index is unusually actionable: it's stable, it's modifiable, and the feedback loop is short enough that you'll see your effort pay off within a single season.
Test once to know where you stand. Adjust your intake based on the result. Test again in three to four months. That's the whole protocol — quietly powerful, and refreshingly free of guesswork.
This article is for educational purposes only and is not a substitute for clinical cardiovascular risk assessment by a qualified healthcare professional. The Omega-3 Index is a useful biomarker, but it should be interpreted in context with your full health picture. If you have a diagnosed heart condition or are under medical supervision, speak with your doctor before making changes to your supplement routine.
Harmover Omega-3 EPA & DHA
180 mg EPA · 120 mg DHA per softgel · Triglyceride form · Stabilised with Vitamin E · 100 softgels
Shop Omega-3 EPA & DHA- Harris, W. S., & von Schacky, C. (2004). The Omega-3 Index: a new risk factor for death from coronary heart disease? Preventive Medicine, 39(1), 212–220.
- Harris, W. S. (2025). Recent studies confirm the utility of the omega-3 index. Current Opinion in Clinical Nutrition & Metabolic Care, 28(2).
- von Schacky, C. (2023). Omega-3 fatty acids in heart disease — why accurately measured levels matter. Netherlands Heart Journal.
- von Schacky, C. (2014). Omega-3 Index and Cardiovascular Health. Nutrients, 6(2), 799–814.
- von Schacky, C. (2010). Omega-3 Index and Sudden Cardiac Death. Nutrients, 2(3), 375–388.
This article is for informational and educational purposes only. Harmover products are food supplements and are not intended to diagnose, treat, cure, or prevent any disease. The Omega-3 Index is not a substitute for clinical cardiovascular risk assessment. Always consult a qualified healthcare professional before making changes to your supplement or medication routine, particularly if you have an existing health condition.